Trigger warning for people with a history of trauma, self injury or other PTSD type issues: this post is about difficult topics and was difficult for me to write and to recover from writing. It may trigger uncomfortable feelings in readers but denial of issues doesn’t help anyone learn how to modify and control the issues for an improved quality of life and/or improved level of self control and safety from self injury. Sexual assault is also a difficult topic but self injury or the urge to self-injure can happen everyday.
“Interestingly, Coleman (1994) studied a group of autistic children who had low levels of calcium (i.e., hypocalcinuria). These individuals often exhibited eye-poking behavior. When given calcium supplements, the eye-poking decreased substantially. In addition, language functioning improved.” [http://www.autism.com/symptoms_self-injury]
— secondary hyperparathyroidism perhaps?
For me secondary hyperparathyroidism can cause significant mental illness symptoms including a feeling of jittery thoughts and a jittery body, with a pent up feeling of needing to pop the bubble – ‘stabby’ feelings with a desire to self injure by stabbing myself. It is extremely unpleasant feeling and at times included a feeling of wanting to pop the eyes – gouge them out. Very unpleasant is an understatement, very dangerous to self is more accurate.
See below for a list of ideas for activities to try to take your mind off the self harm urges, and book reference written for health professionals rather than for a patient or parent – but help is help which can be life saving when needed.
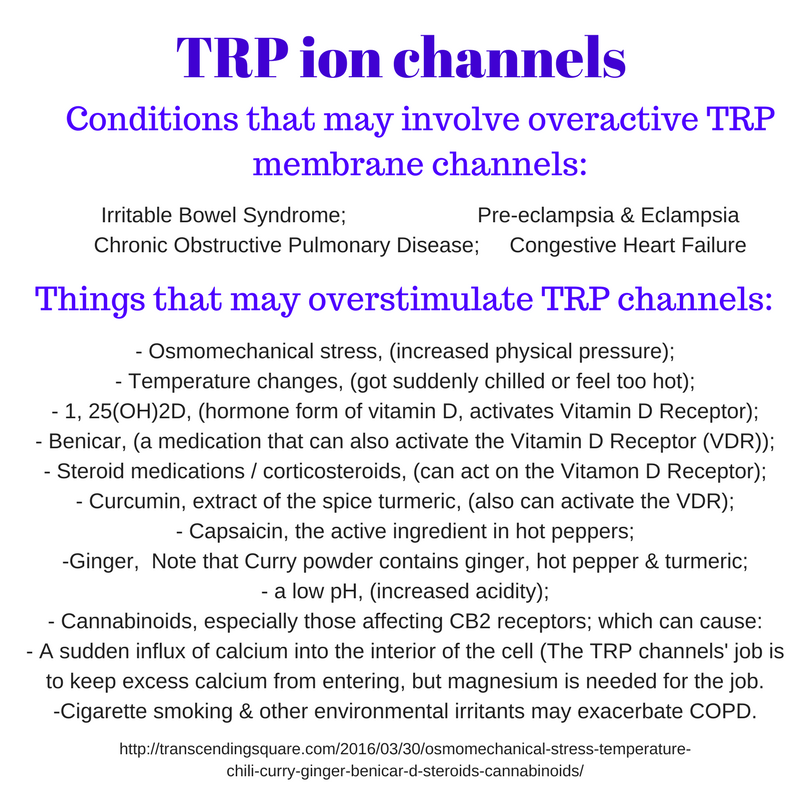
Secondary hyperparathyroidism can be caused by low vitamin D or low calcium. My endocrinologist was extremely insistent that I take both vitamin D and calcium but over the years I had learned, with lab test proof, that my hormone D tends to be in the elevated end of the normal range. Irritability to an excessive level can occur at the elevated end of the range of hormone D. Lab test ranges are just based on the averages that are seen by the lab — and lab tests are usually ordered for sick people not for healthy people, so those lab test ranges are really the range of values seen in sick people not a range based on the average values seen in only healthy people.
I didn’t comply with the endocrinologist’s recommendation and found that just increasing calcium intake stabilized my level of parathyroid hormone and took away the ‘stabby’ feelings.
It is common for corticosteroid balance to be different from normal in patients with autism. [see link below] Vitamin D and hormone D are actually seco-steroids and the active hormone D acts somewhat like steroids in the body. Autism patients may be like people with obesity and many other chronic illnesses, that have been associated with low vitamin D but supplements weren’t found to be helpful for the various conditions. The problem may be more like mine where I have too much hormone D which is converted from vitamin D, and which leads to low levels of vitamin D. [http://www.preventmiscarriage.com/documents/Immunological-Considerations.pdf]
Vitamin D is carried on a transport protein that acts to keep it inactive. When free within the body the vitamin form is quickly activated to the hormone form. There are many more Vitamin D receptors throughout the body than there is usually enough hormone D to activate them all during states of normal health.
Autism and other chronic diseases that seem to associated with low lab test levels of vitamin D may actually be reflecting a problem or deficiency in the vitamin D carrier protein rather than representing an inadequate amount of vitamin D being supplied from the diet or an inadequate amount of time spent in direct sunshine. Vitamin D is based on cholesterol and is not actually an essential vitamin in the way that other vitamins are essential because our bodies can make vitamin D from cholesterol when we get about 15 to 30 minutes of sunshine per day on our face, throat, and bare arms.
Magnesium baths help circumvent the problem elevated hormone D causes within the gastrointestinal tract — calcium is absorbed preferentially and magnesium deficiency can result which also can be a cause of significant irritability.
Providing nutrition education and individualized nutrition care in the public health sector is where I have training and experience. — ie giving away free information. Making money is not where I’ve had experience. And traveling has proven to be difficult for me with my various autoimmune and food sensitivities, but I care a lot about pain and suffering and mental anguish, in myself and others.
It is unpleasant to have to feel an urge to hurt oneself, and it is hard to control an internal explosive feeling that has nothing to do with how your childhood went — talk therapy is not much help if the problem is actually hyperparathyroidism. Multiply that internal jitteriness and explosive feeling by days, months, or years, and it is really much better to take calcium supplements and magnesium baths then to talk to a therapist about your childhood — while trying to control the urge to poke yourself in the eyes. (They don’t understand, and the endocrinologist didn’t either. Lab tests are just lab tests and mood symptoms are referred to a psychiatrist for mood stabilizing medications – in my (bad) experience.)
- Autistic kids wash up happier in an Epsom salt bath, .
- I describe my current Epsom salt bath routine towards the end of this post: Substance P, neuropathic pain, migraines, and the cannabinoid system,
The way “fair use for educational purposes” works is that the information is provided not for profit. I share information, which may contain excerpts from copy-righted works, in the hopes that some individuals or clinicians will find some of the information helpful, and to keep within the guidelines for fair use I don’t ask for donations or charge money for the information.
(Brief excerpts fit the guidelines better, the Autistic kids wash up happier post was a post from years ago, before I had learned more about fair use guideline. It contains an extensive excerpt from a much longer article, but it is very helpful information regarding some special dietary needs that are common among children with autism and which I also found helpful for improving my own diet. I have recently found that I have several genetic defects that are also commonly found in children with autism. One of them affects two important amino acids so that might be a problem that could affect my ability to make the vitamin D carrier protein – but I haven’t looked into that metabolic pathway yet.)
Ideas for activities to substitute if feeling an urge to self harm; from the book “Treating Self Injury, A Practical Guide,” by Barent W. Walsh, Ph.D. (2006) written for mental health counselors or psychologists:
https://www.guilford.com/books/Treating-Self-Injury/Barent-Walsh/9781462518876
- Negative Replacement Behaviors – a preliminary step, a substitution behavior that represents the typical method used – if actual self injury is already a problem. For example drawing a red mark instead of cutting, pounding a pillow or something else instead of hitting oneself.
- Mindful Breathing Skills – we tend to hold our breath in stressful situations and lack of oxygen makes rational thinking and self control more difficult.
- Visualization Techniques- visualize a happy place or memory or some other practiced calming scenario.
- Physical Exercise – use up the pent up energy in real exercise instead of mental or physical pain.
- Writing – journaling about things you are grateful for can help sometimes to see that life is worth it even though difficult too. Journaling about worries sometimes can help work through to solutions.
- Artistic Expression – art in many forms can help work out unspoken memories or feelings.
- Playing or Listening to Music – frequencies and rhythms can be healing or unsettling .
- Communicating with Others – phone a friend, counselor, or hotline or make a private audio journal.
- Diversion Techniques – escapist type behaviors to fend off or delay self injurious behaviors rather than try to feel that they must be confronted or solved immediately – just don’t want to deal with a band-aid right now so will draw a picture or go for a walk or call a friend – sometimes pausing is enough to let the urge fade.
* The capitalized techniques are from the book, the longer explanation is my interpretation or paraphrase of the book’s discussion of the topic. These notes are from notes I copied down years ago when I was having symptoms and hadn’t yet learned of the hyperparathyroidism condition.
“Treating Self Injury, A Practical Guide,” by Barent W. Walsh, Ph.D. (2006): https://www.guilford.com/books/Treating-Self-Injury/Barent-Walsh/9781462518876
The website provides a pdf link for a 25 page practical guide with Reproducible Materials for treating self injury. It includes client screening forms, safety contract, and an extensive section on breathing techniques for self calming. https://www.guilford.com/add/forms/walsh5.pdf
/Disclosure: This information is provided for educational purposes within the guidelines of fair use. While I am a Registered Dietitian this information is not intended to provide individual health guidance. Please see a health professional for individual health care purposes./
*update 8/13/2022
For updating –
https://twitter.com/deNutrients/status/1101527023661522945