
My incomplete paper led to further discoveries about the role of bitter taste receptors in kidney health and it involves butyrate and the niacin GP109 receptor.
12330 words, what can I say, I forgot the Conclusion section too. I learned new things, though, and need to modify the Abstract now to include the new insights and additional topics. The post is long, and the Reference List is elsewhere and needs to be collated. The first half of the paper about the causal factors that may be involved in histamine excess and Retinoid Toxicity was written from memory based on the schizophrenia research series I wrote earlier in the summer, and that part needs more citations. First post in that series: Schizophrenia risk factors may also be Alzheimer’s risk factors; Experimental design and variables. (substack.com) on the series on this Substack and needs more citations.
Addition: I got an extension on the deadline, a month, maybe I will make it after all!
Working Title: Pomegranate phytonutrients for mast cell inhibition to reduce the pain and suicide risk associated with histamine excess in neurologic conditions, drug related akathisia or post infection illness.
(Initial) Abstract
Multifactorial Problems need multifactorial solutions – Retinoic acid deficiency or excess and histamine excess are seen in many neurological conditions including schizoaffective disorders, FAS, ADHD, autism spectrum disorder and Alzheimer’s dementia; and in ME/CFS following Epstein-Barr Virus. ME/CFS has been seen in Covid19 survivors. Attempts to use histamine antagonists or reverse agonists for symptoms of histamine excess have had limited success due to adverse effects from peripheral Histamine receptors. (Cheng et al, 2021) Instead of the side effect risk of histamine receptor antagonists, reducing the level of histamine could provide improved quality of life and reduce the acute mental and physical pain of excess histamine levels – which can range from seasonal allergies and migraines to emotional dysregulation with risky behavior or severe anxiety, to suicidal urges and self-harm. Histamine and retinoid excess can occur daily for sufferers as many common foods add to the risks. Long term risks of chronic Retinoid toxicity and/or histamine excess include kidney, liver, and brain damage. Osteoporosis and pancreatic problems may also occur. Use of vitamin A or retinoids has also had mixed results – some patients may have low levels while others may have an over-activation of Retinoic Acid occurring and supplements would worsen their symptoms. Evaluating why individuals have excess histamine is needed so targeted care can be provided to reduce the degranulation of mast cells and release of histamine or mitigate for other genetic differences affecting retinoid metabolism or the histaminergic system that lead to a tendency towards histamine excess. Histamine excess can lead to hippocampal damage over time. NMDA receptor antagonists can be protective in addition to antihistamine medications.
Multifactorial solutions are needed. Polyphenols in pomegranate fruit or peel, and other produce with quercetin and luteolin, can provide short term help for acute symptom management, and help maintain a lower inflammatory lifestyle over the long term. The polyphenols in pomegranate reduce the histamine symptoms within a short time frame by inhibiting mast cells or modulating the inflammatory cytokines that are also released during degranulation. Having a two to three-ounce serving of pomegranate juice or seeds twice a day can be inconvenient and expensive. Treatments made with the more potent peel can be produced inexpensively for year around use (pomegranate is a seasonal fruit). The tannin content of the outer peel is a factor that adds diuretic effects, which is helpful for detoxification but may limit medicinal use of whole peel products except as an extract or for use in milligram amounts. The inner pith includes tannins but in a lower ratio and can be used as an antioxidant food preservative, as a bitter, tangy flavoring, or as a gelling agent. Pomegranate products also promote microbiome health and improve symptoms of Metabolic Syndrome. Postbiotic metabolites may be formed from pomegranate phytonutrients that can cross the blood brain barrier, reduce neuroinflammation and may promote regrowth of hippocampal cells. Mineral chelation properties promote antimicrobial and anticancer effects (with reduction of metastasis risk in particular) and chelation of other toxins and adsorption of nanoparticles. Pomegranate as a whole fruit product includes multifactorial solutions that protect health and mood in many ways.
Clinical trials are needed which assess all participants for underlying causal factors prior to beginning an experimental or control phase of the study. Excluding all people found with underlying confounding variables would not work for conditions that are considered heterogenic – the condition itself is variable. Monitoring and treating the identified variables in a self-controlled case study that compares the patients to their own progress or degeneration over time (Gault, et al, 2017) (Heinrich, et al, 2020) might be a way to research multifactorial conditions that may involve many varied gene alleles, different nutrient deficiencies or imbalance, and which lead to microbiome and mitochondrial dysfunction. The order treatments are provided can also impact their effectiveness. Restoring nutrient balance and underlying function, may be needed before some treatments may be able to help.
Introduction
Histamine excess and/or retinoic acid excess may be causal in many neurological conditions (Fernández-Novoa et al, 1994) including schizoaffective disorders, FAS, ADHD, autism spectrum disorder and Alzheimer’s Dementia. Both issues can cause pain ranging from seasonal allergies to severe mental illness – both can lead to histamine hyperexcitability with emotional dysregulation. Self-injury, panic, anxiety, suicidal urges, or mania and reckless behavior can occur and may be diagnosed as schizophrenia or bipolar disorder Type 1 and be treated with psychiatric medications that would not reduce histamine levels. See Table 1. Symptoms of Histamine Excess and of Retinoid Toxicity.
Histamine excess can cause severe mental symptoms that may include suicidal urges – daily if the excess histamine levels are present daily. Suicide is a risk in schizophrenia yet other chronic damage on average causes death more often in the cohort. The histamine excess causes inflammatory symptoms throughout the body and targets the hippocampus which may lead to an Alzheimer’s diagnosis later in life. Histamine functions as a neuromodulator, excess leads to hyper-escalation of brain activity and mood whether anxious fear or manic grandiosity, which leads to an increase in mitochondrial workload and oxidative stress chemicals. Extra antioxidants and cofactors would be needed or worsening of mental health symptoms is likely as nutrient deficiencies become severe.
Histamine excess is debilitating physically and mentally, and chronically can lead to hippocampal damage and Alzheimer’s dementia.
- Histaminergic abnormalities or histamine excess are seen in many neurologic conditions.
- Pain may vary from minor seasonal allergies and inflammation to more severe mental psychosis and self-injurious behavior or suicide risks.
- Current treatment use of antihistamines or reverse agonists for narcolepsy have had side effects of sleepiness or peripheral histamine receptor side effects. (Cheng et al, 2021)
- Currently diagnosis of histamine excess problems may be inconclusive, yet the problem may be ruled out based on the lab tests for DOA enzyme or histamine levels.
- More effective screening and treatment methods are needed for acute treatment during histamine excess and for prevention of chronic degeneration over time.
The problem of histamine excess is multi-factorial with varied potential causal factors which would need targeted treatment specific for each individual or group with a similar cluster of causal risks. Thorough screening would be needed to identify genetic differences affecting digestion or metabolic pathways, nutrient imbalance, and lifestyle variables that may affect mast cells or stress. Varied treatments would then be needed to mitigate for each of the identified potential causal factors. Treating only one or a few might leave enough causal issues that symptoms remain. Gradually working through a list might make it possible to eventually restore optimal function and improve the patient’s quality of life – if the improvements continue on a daily or frequent enough basis to prevent a return of histamine excess in the diet, or nutrient imbalances, or excessive mast cell degranulation – or all three.
The diagnostic tests for histamine excess or mast cell over activation can be inconclusive. Retinoic acid levels may need to be checked in specific tissue locations as the over activation may be localized. In chronic alcoholism the liver over activates Retinoic acid and transports it elsewhere in the body leading to deficiency levels in the eyes and liver and excess in the testes* (*drinking by males prior to conception is a link between FAS and ADHD) and elsewhere. Less is known about over-activation continuing after a viral infection (EBV (Jones, et al, 2007), possibly SARS-CoV-2 (Bonilla, et al, 2022)) and causing the varied symptoms of ME/CFS.
Over activation of vitamin A or carotenoids to Retinoic acid may become a lifelong problem after prenatal alcohol exposure, or immune challenge from certain viral infections (Epstein Barr Virus (Jones, et al, 2007) and possibly SARS-CoV-2. (Bonilla, et al, 2022), (Mawson et al, 2021) Vaccine injury and other drug related chronic symptoms including akathisia may also be related to retinoid excess related to liver injury. (Mawson, Croft, 2020)
Retinoic acid excess would cause mast cell degranulation and increase histamine. It can lead to liver and kidney damage in addition to neurocognitive degeneration risks and other chronic pain symptoms of seasonal allergies, migraines, skin rashes, bone spurs, and inflammation. Histamine excess may then be more of a risk and symptoms may occur intermittently based on varying intake of vitamin A rich meals or supplements or use of topical retinoid products.
Histamine hyperexcitability might then also be intermittent with extreme fear or mania happening due to liver dinner and peach cobbler the day before. Pomegranate polyphenols might help during the episode but knowing to avoid vitamin A and histamine foods in the first place would be better. And TRP activating foods or substances and activities is a new therapeutic diet strategy included in Table 2. Potentially Inflammatory Food Categories. TRP channel activators are common in spicy foods and other condiments. They may also be a causal factor for pain from migraines and IBD/colitis and add to the effects of histamine excess, hyperinflammation, and the increased oxidative stress may lead to mitochondrial dysfunction. This Table is a small sample of a much larger database that would be helpful for patients and clinicians to have created. It is discussed in a later section.
Lifestyle and diet change needs are provided in Table 3 as an example of the many variables that can worsen chronic inflammation and increase mast cell degranulation; Table 3. Self-Care Patient Guidance for ME/CFS, hyperinflammation, Retinoid Toxicity and/or histamine excess.
The nociceptive pain of histamine excess can be dry, itchy eyes, puffy, painful body, and a runny nose, but it also might be irrational mental symptoms leading to self-injurious behavior or sexual recklessness. The emotional dysregulation can lead to escalation of whatever feelings the person is experiencing. Table 4. Counseling Strategies for Coping with Urges to Self-Harm has distraction and other tips for patients with dissociative or self-injurious issues.
ME/CFS, fibromyalgia, MCAS, Ehlers-Danlos Syndrome (EDS), Dysautonomia or POTS, can all be chronic and comorbid problems with little help available regarding reversing the symptoms. Histamine excess and/or Retinoid Toxicity might be underlying factors. Lack of cannabinoids due to genetic differences or antiphospholipid syndrome might be a factor. Other nutrient deficiencies or a high saturated fat diet might be factors adding to mitochondrial dysfunction. Treating symptoms instead of underlying causal factors leaves the patient with some pain and symptoms and ongoing chronic degeneration is likely continuing. Medications may also have negative side effects.
Histamine excess symptoms also add a risk of the person being prescribed psychiatric medications as the hyperexcitability episodes can appear manic, delusional, and/or angry and dangerous. Psychiatric medications can increase risk of nutrient depletion and may lead to worsening symptoms over time which may be diagnosed as schizoaffective disorder and more medications may be prescribed. Mitochondrial support nutrients, risk factors for schizophrenia and nutrients depleted by commonly prescribed psychiatric medications have many in common. See Table 5. Nutrients depleted by common psychiatric medications and nutrients that may be deficient or imbalanced in patients with schizophrenia/schizoaffective disorder and mitochondrial support nutrients – all overlap. With underlying causal factors remaining unidentified and untreated, the ongoing degeneration may then lead to Alzheimer’s dementia. Histamine excess targets the hippocampus which is the area with more severe damage in Alzheimer’s.
Table 6. Genes that may be involved in Retinoid Toxicity or Histamine excess – is a start but incomplete.
Pain is a signal from our body that we are doing something wrong, or something is inherently wrong due to metabolic differences. Pain medications to block or desensitize pain leave the body vulnerable to ongoing damage. Chronically low magnesium can be causal for hypertension and Type 2 Diabetes and chronic pain conditions such as migraines. Identifying the causes of pain and removing them or mitigating for them, reduces both the daily pain and long-term risk of chronic damage from inflammation.
Pharmacology products and pomegranate products can help mitigate pain and inflammation, while knowing what to have for dinner can help prevent pain and inflammation the next day, or suicidal urges and the emotional dysregulation of histamine hyperexcitability.
Pomegranate related Tables:
- Table 7. Health benefits observed with pomegranate products. *incomplete.
- Table 8. Phytonutrient content of Pomegranate products and extraction methods. *incomplete. Tables regarding antimicrobial research combines what I was attempting in Tables 7 and 8. Their Tables include which species were targeted using pomegranate extract, standardized to 13% ellagic acid, or other extraction methods are listed. (Celiksoy and Heard, 2021) It is a Chapter in an open access peer-reviewed book: Pomegranate, IntechOpen, 2021.
- Table 9: Topical and Pharmaceutical trials with Pomegranate products.
- Table 10. Research with pomegranate peel as a food preservative or ingredient.
- Table 11. Industrial applications with Pomegranate peel.
Causal factors for histamine excess seen in neurological conditions may include:
The causal factors are numerous and variable as many gene alleles may be involved, and the at-risk population seems to have numerous varied gene differences impacting their metabolism. Metabolic pathways affected by a dysfunctional or overactive gene allele can sometimes be helped by diet changes or supplements. Identifying the differences is a need though. A summary of potential risks is included in Table 12. Potential Causal factors for histamine excess or Retinoid Toxicity.
Genetic heterogeneity with multiple metabolic gene alleles that leads to a similar phenotype of histamine excess. Congenital SNPS may be varied and in multiples.
- Low methylation or a difference in the DOA enzyme might be causal factors treated with methylated forms of folate and B12 and choline, or supplements of the enzyme DOA which breaks down histamine.
- Other gene differences might decrease ability to reduce oxidative stress and the resulting inflammation risk could lead to more degranulation of mast cells and release of histamine.
- Endocannabinoid deficiency or imbalance due to genetic differences can be causal as both the THC and CBD equivalents, anandamide and 2-AG, are needed to inhibit a mast cell from degranulating. (BHMT gene is an example).
- Retinoic acid, the active form of vitamin A, is involved in immune function and can cause degranulation of mast cells and add to an histamine excess problem. Over activation of vitamin A or carotenoids to Retinoic acid may be a gene difference that can result from Fetal Alcohol exposure from the sperm arriving with alcoholic DNA damage, or prenatal alcohol use. Alcohol use in an adult affects retinoic acid activation leading to low levels being present in the liver and eyes and increased transport from the liver to other areas of the body including the testes.
- Vaccine injury. (Mawson, Croft, 2020); certain viral infections (Epstein-Barr virus (EBV) (Jones, et al, 2007) and SARS-CoV-2 has led to similar ME/CFS problems as seen in EBV survivors, (Bonilla, et al, 2022), liver injury leading to excess retinoids may be involved (Mawson et al, 2021); and possibly the drug/withdrawal reaction referred to as akathisia (~restless legs, but it can include mental symptoms), may also lead to an ongoing increase in the liver activation of carotenoids or vitamin A to the active Retinoic Acid form. From the liver the Retinoic Acid is sent out to the body on transport proteins.
Diet related factors:
- Diet is a source of histamine. Reducing use of histamine food sources or foods that increase mast cell activation in the gut may make a very significant improvement in symptoms. Other inflammatory or allergy promoting foods would also be causes of mast cell degranulation.
- If Retinoic Acid overactivation was found to be a problem, then strictly reducing vitamin A and carotenoids in the diet may also be needed for significant improvement to be seen.
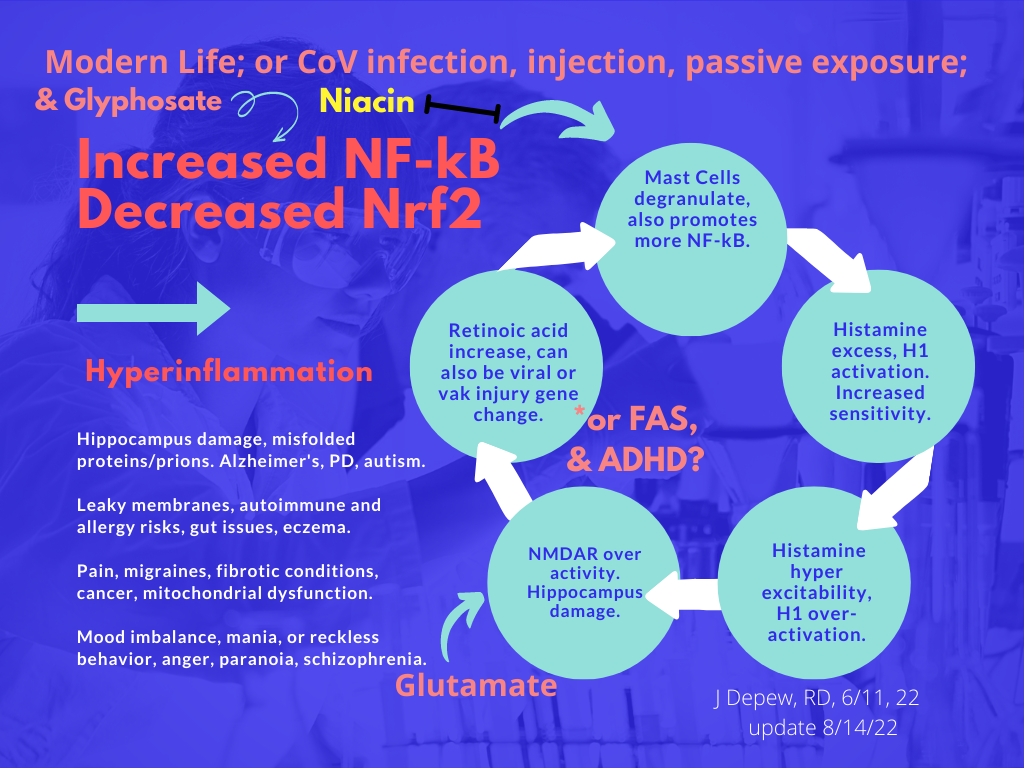
- Glyphosate increases inflammatory Nf-kB which reduces anti-inflammatory Nrf2 and adds to the degranulation of mast cells and may negatively affect the microbiome, leading to other inflammatory signaling.
Other lifestyle or trauma history factors:
- Circadian cycle abnormalities; EMF or radiation sources, (Rusin, et al, 2021); flickering lights/strobe light like effects in media; and stress whether physical or emotional; are also able to cause degranulation of mast cells and exposure the day before may lead to a migraine the morning after spending time seeing strobe light effects (went to see an action movie last night). Wearing dark sunglasses can protect against the flickering light trigger.
- Psychosomatic symptoms or trauma history may be a factor as emotional or physical stress can add to the mast cell activation. (Baldwin, 2006) In schizophrenia psychosomatic symptoms were not found to be that common which was taken to suggest that there is a biologic basis to the condition. Identifying and working through any emotionally caused symptoms may be needed in addition to other strategies to restore optimal quality of life as the emotional pain could be adding to histamine excess too, due to the degranulation of mast cells. (Baldwin, 2006)
The summaries above are likely not all inconclusive but begin to show the complexity of potential causal factors for histamine excess and/or Retinoic Acid excess. See: Table 12. Antihistamine medications can help dampen some flames of excess histamine but blocking receptors will not stop the influx of more histamine from dietary sources, or histamine that lifestyle and stress may be adding each day from mast cell degranulation.
Conditions seen as Comorbid with ME/CFS.
- Ehlers-Danlos Syndrome (EDS) is seen as a comorbid condition with ME/CFS. Gene differences affecting collagen production lead to varied symptoms of pain, joint instability, and fragile blood vessels and skin. The variations of EDS are currently grouped into 13 types. (ehlers-danlos.com/what-is-eds/)
- Dysautonomia may also be comorbid with ME/CFS, often seen as Postural Orthostatic Tachycardia Syndrome (POTS). Anti-phospholipid autoimmune antibodies may be a cause of POTS, (dysautonomiainternational.org/page.php?ID=150), and has been seen in patients with LongCovid symptoms. Both antiphospholipid syndrome (APS) and COVID-19 are theorized to have similar microvascular injury preceded byendothelial damage, complement activation, and formation of neutrophil extracellular traps “(Netosis).” (Wang X, et al, 2021) Pomegranate peel phytonutrients could help by inhibiting NET formation. (Kirchner, et al, 2013)
- Fibromyalgia may also be comorbid with ME/CFS and involves fatigue and widespread pain. The cause is unknown. *My everything hurt – retinoic acid toxicity symptoms felt similar to fibromyalgia for me (n =1) for a day or two after accidentally eating ¼ of a peach. Patients with fibromyalgia are described as being more sensitive to pain by the CDC webpage, they may be experiencing more pain than normal, and throughout the body simultaneously. (cdc.gov/arthritis/basics/fibromyalgia.htm)
- Mast Cell Activation Syndrome (MCAS) is also seen as a comorbid condition with ME/CFS. It involves histamine excess due to overactive mast cell degranulation, with increasing sensitivity to number and amount of trigger foods and changes in temperatures which suggests TRP channels are involved. Increased expression of TRP channels has been observed in inflammatory bowel conditions.
“Specific triggers and symptoms of MCAS vary greatly between individuals, and additional triggers can include fragrances, exercise, stress, and changes in temperature. MCAS symptoms can be episodic (come and go) and may often change over time within the same person. This can make it difficult for people with MCAS to identify their specific triggers, and the number of triggers and severity of symptoms may continue to increase as the condition progresses.” (mastcellaction.org/about-mcas)
- ME/CFS Comorbid condition list: (Young, 2022)
Females are more likely to have fibromyalgia and may be more sensitive to pain due to TRP channels that have a narrower sensitivity range. Males needed four times more capsaicin on average than females to have a similar reaction, (Lu et al, 2009). (Artero-Morales, et al, 2018)
Pomegranate products can help acute symptoms and reduce or mitigate long term risks of histamine excess and Retinoid Toxicity.
Pomegranate products can help reduce the short-term effects of histamine excess by reducing inflammatory cytokines, promoting Nuclear factor E2 related factor (Nrf2) and inhibiting mast cells from degranulating and releasing more histamine. Histamine and other inflammatory chemicals activate TRP channels which can lead to pain and edema and a runny nose. In greater excess histamine may cause irrational fear or mania and suicidal urges as it impacts dopamine levels and CNS function. Pomegranate benefits can also help reduce long term risks from histamine excess of inflammatory damage to the brain, liver, and kidneys. (Table 1. Symptoms, Table 7. Benefits of Pom) Promoting Nrf2 is promoting immune function, DNA damage repair, and glutathione production and Nrf2 also inhibits mast cell degranulation. Pomegranate contains antioxidants and promotes our own production of glutathione and other antioxidants by promoting Nrf2. Histamine excess or Retinoid Toxicity both can lead to neurological, hepatic and renal fibrosis and scarring. (See Table 1.) Retinoid Toxicity causes histamine excess but also has more extensive negative impacts on health and prenatally is a teratogen. Pomegranate phytonutrients can provide relief for acute symptoms of histamine excess while also promoting a healthy microbiome, supporting mitochondrial DNA and their function, and reducing risks of liver, kidney, or brain damage. Urolithin A and B are microbiome metabolites of pomegranate phytonutrients, which can cross the blood brain barrier, reduce neuroinflammation, and promote hippocampal neurogenesis. (See Table 8. Pom Phytonutrients.)
Nrf2 promotes SIRT-4 which inhibits mast cell degranulation by inhibiting the metabolism of their mitochondria. (Hu B et al, 2020)
The acute symptoms of histamine excess can be life threatening as suicidal urges or reckless behavior may occur. Histamine hyperexcitability episodes may be more likely to occur when overly tired, hungry, or emotionally charged. Practicing calming strategies, breathing techniques, mantras, and other distractions in advance can help at the time of need when thinking is irrational. Table 4. Counseling Strategies for Coping with Urges to Self-Harm provides examples of patient guidance talking points or for use in a handout. Specific guidance from an authority figure that self-harm is not okay and that the patient is worthy of help and care from others, and themselves, might help prevent a tragedy. The irrational recklessness needs to be paused long enough for the person to remember to try the pomegranate product, quercetin, luteolin or other medications or call a referral phone number.
Polyphenols from pomegranate and other produce sources of quercetin or luteolin can help inhibit mast cells and reduce symptoms of histamine excess. Pomegranate peel extract was found to inhibit NF-kB. (Rasheed, et al, 2009) Punicalagins, hydrolyzable tannins from pomegranate peel, can act as a modulator of the NF-kB signaling pathway, which would prevent inflammation. Doses of 50, 100, and 200 mg/kg of pomegranate peel extract were used in an animal-based model of arthritis, compared with the NSAID medication indomethicin. The 200 mg/kg dose of pomegranate extract was found to reduce pain and inflammation with downregulation of TNF-R1, TNF-α, IL-1β, IL-6, NF-κB, reduction in oxidative stress markers and improved tissue histology. (Karwasra, et al, 2019) Pomegranate mesocarp decoction (300 mg kg−1), or polysaccharides (300 mg kg−1), or ellagitannins (45 mg kg−1) reduced visceral hypersensitivity from drug induced colitis in an animal model by inhibiting mast cells. The polysaccharide portion was not as helpful as the pomegranate decoction or dose equivalent ellagitannins, however it was beneficial. (Parisio, et al, 2020)
Nociceptive pain improved significantly more with combined use of pomegranate peel extract and aspirin than the theoretical ED30 with a benefit of reducing negative effects of aspirin. The mechanism of action of the synergistic treatment “involves the l-Arginine/NO/cGMP pathway, antioxidant capacity, and high content of total phenols.” (Guerrero-Solano, et al, 2021) Pomegranate peel acts as a modulator of Nitric oxide (NO), with phytonutrients that can up or down-modulate Nitric oxide production by affecting eNOS or iNOS.
Nitric oxide modulator – Pomegranate phytonutrients are modulators.
Pomegranate extract has been shown to reduce pain and inflammation by the same mechanism as NSAIDS – inhibition of cyclooxygenase enzymes (COX1 and COX2, with more inhibition of COX2 than COX1). It also may have an anti-inflammatory effect by reducing inflammatory cytokines that signal increased production of Nitric Oxide (NO) and Prostaglandin E2 (PGE2). (Shukla, et al, 2008) Prostaglandin E2 is made from arachidonic acid and is involved in the inflammation associated with rheumatoid arthritis and osteoarthritis. (Jean, et al, 2006)
Pomegranate extract was found helpful in a dose related level against mammary tumerogenesis in an animal study, (0.2-5 gram/Kg body weight was used). Reducing COX2, heat shock protein 90 (HSP90), nuclear factor-κB (NF-κB) pathways and increasing Nrf2 pathways were found to be part of the mechanism for benefit. (Mandal, et al, 2017)
Pomegranate peel phytonutrients have modulatory benefits for coping with oxidative stress and can help increase low levels of Nitric oxide (NO) by promoting eNOS (Delgado, et al, 2017), (de Nigris, et al, 2007a), (Monsalve, et al, 2017) (Wang D, et al, 2018), or reduce excess NO by promoting iNOS. (Kandeil, et al, 2019) (Guerrero-Solano, et al, 2021)
Nitric oxide can be beneficial but in excess it can also transform into reactive oxidative species and add to the antioxidant burden of metabolism. (Matsubara, et al, 2015), (Aouache, et al, 2018) Other studies including an animal study on obesity found pomegranate extract reduced inflammatory biomarkers and increased nitric oxide, which might make it helpful for Metabolic Syndrome. (de Nigris, et al, 2007) Pomegranate has modulatory benefits, helping increase nitric oxide, or decrease it, as needed, via effects on iNOS and eNOS. Different phytonutrients within the peel may be involved in the varied actions. Hydrolyzable tannins within pomegranate peel including punicalagin and punicalin, “have an inhibitory effect on NO production, COX-2 expression and PGE2 [28].” (Guerrero-Solano, et al, 2021)
Improved endothelial function in the placenta was seen in an animal model for diabetic pregnancies using pomegranate extract; eNOS -/- knockout mice and wild-type were used. (El-Sayyad, et al, 2019)
Overview of the benefits and mechanism of action of pomegranate peel extract.
There are many excellent reviews of the benefits and safety of pomegranate peel extract – dosage matters – larger doses are more of a risk to health and are effective against cancer cells with less risk to patients than typical chemotherapy or other cancer treatments. The strong anti-inflammatory effect of pomegranate peel in “ovalbumin-induced asthma in mice [27]” (Čolić, et al, 2022) is pertinent to my own health as autoimmune sensitivity to eggs seemed to be the cause of new onset of symptoms for me after a particularly stressful time in my life. I stopped use of eggs and eventually all animal products and hemp kernels (plant version of albumin) which helped relieve the skin breakdown that had occurred.
“Oxidative stress, apoptosis, and autophagy are tightly associated with inflammation. In this context, numerous in vitro and in vivo experiments have shown that the pomegranate extract exhibits a strong anti-inflammatory effect [1,2,12]. The effect was confirmed in models of ulcerous colitis [20–22], rheumatoid arthritis [23,24], neuroinflammation [25], skin inflammation [26], ovalbumin-induced asthma in mice [27], lipopolysaccharide (LPS)-stimulated RAW264.7 macrophage cells [28], human neutrophils stimulated with formyl-methionyl-leucyl-phenylalanine (fMLP) and phorbol myristate acetate (PMA) [29].
Similar anti-inflammatory findings were observed in patients with rheumatoid arthritis [30,31] and inflammation in patients with unstable angina or myocardial infarction [32],
obese persons [33], or hemodialysis patients [34]. The investigated parameters depended on the goal of the studies, but most of them were associated with decreased production of proinflammatory cytokines such as interleukin-6 (IL-6), IL-1β, tumor necrosis factor-α (TNF-α), NO, prostaglandin E2 (PGE2), or polarization of pro-inflammatory M1 macrophages into
anti-inflammatory M2 macrophages [1,2,35,36]. The most investigated signaling pathway
involved nuclear-factor kappa B (NF-κB) and cyclooxygenase-2 (COX-2) [35,36].” (Čolić, et al, 2022, CC By the authors.)
Pomegranate peel extract has antioxidant effects at low doses and can be a pro-oxidant at large doses. UVB-induced oxidative stress was inhibited in keratinocyte HaCaT cells at a dose ranging from 2.5-40 µg/mL. Doses ranging from 100-200 µg/mL caused oxidative stress in leukemia and fibrosarcoma, and lung cancer cell lines, leukemia and fibrosarcoma. (Čolić, et al, 2022)
Pomegranate phytonutrients have immunomodulatory effects and may up or down regulate activity.
“The anti-inflammatory effects of pomegranate and its constituents have been demonstrated in various experimental models and human diseases [28,74,75]. In a summary of a recent review, Baradaran Rahimi et al., 2020, emphasized that pomegranate and ellagic acid modulate the inflammatory process by reducing many inflammatory cytokines and chemokines such as TNF-α, IL-1β, IL-6, IL-8, and IL-18. The target signaling molecules, receptors, or transcription factors include COX-2, NF-κB, Janus kinase (JNK), inducible nitric oxide synthase (iNOS), P38, extracellular signal-regulated kinase (ERK), Nrf2, peroxisome proliferator-activated receptor (PPAR)-α, and PPAR-γ [1]. We tested the modulatory effect of PoPEx on only two proinflammatory cytokines from the innate cytokine family (TNF-α and IL-6) in PHA-stimulated PBMC cultures and confirmed previous findings. TNF-α was inhibited by both lower and higher PoPEx concentrations, whereas inhibition of IL-6 was seen only at higher doses. The differences could be due to the fact that under certain conditions, IL-6 may also have an anti-inflammatory role [76].” (Čolić, et al, 2022, CC By the authors.)
PPAR receptors can be activated by a form of vitamin A, 9-cis-Retinoic Acid, (Tate, et al, 1994), and cause mitochondria to switch to fermentation of fat instead of using the more efficient and less waste producing Citric Acid Cycle, which will be discussed more later. ERK causes phosphorylation of proteins which in excess may add to hypersensitivity of pain conditions by post-translational modification (PTM) of ion channels or other proteins, (Tingting, et al, 2019), which leads to autoimmune or other dysfunction. PTM will also be discussed later. Other types of post-translational modification also can occur – glycosylation of hemoglobin is an example. Reducing the occurrence of PTM would be beneficial for nociceptive and chronic risks.
TRP channels, nociceptive pain and endocannabinoid breakdown in hyperinflammation.
A discussion of histamine and nociceptive pain requires discussing TRP channel activators and dysfunction. TRP channels are involved in sensory perception and nerve signaling – communicating the perception, and control of cells – responding to the perception. The response might be nociceptive or neuropathic pain signals or many other functions. There are many types of TRP channels that do varied things in response to a variety of stimuli and can have different actions depending on the ligand.
The TRP pain chain of events: emotional or physical stressors lead to the degranulation of mast cells, which release histamine and cytokines, which activate TRP channels that send pain signals via an increase in intracellular calcium or sodium, or other functions occur that may result in mucus flow or tissue edema. The influx of calcium can lead to overactivity of a cell and lead to cell damage and may add up to cell death (Kumar, et al, 2013) and fibrotic damage over time.
TRPV1 – nociceptive pain signaling and anti-inflammatory roles.
Vanilla/vanillin is calming. The TRPV1 channels can do anti-inflammatory things or send pain signals depending on the agonist. Trials with antagonist medications led to negative side effects due to the many peripheral functions of TRPV1 channels. Avoiding the TRP activators helps avoid the pain or colitis flare-up.
TRPV1 is a type of ion channel that includes as agonists: histamine, capsaicin and the endocannabinoids anandamide and N-arachidonoyl-dopamine as agonists, also temperatures above 43’C and acidic pH conditions below 6.0 can cause a burning pain sensation. (Silverman, et al, 2020) Males can tolerate more capsaicin than females on average, four times more to achieve the same stimulus. (Artero-Morales, et al, 2018) Vanillin is an agonist with calming effects. TRPV1 channels are also found in microglia of other brain regions associated with pain including the thalamus, somatosensory cortex, periaqueductal gray (PAG) and hippocampus but are not typically found on microglia. (Marrone, et al, 2017) TRP channels are varied in type and function and sense the environment for different cell types. They are involved in pain signaling C and Alpha-delta sensory nerves of neurons in the spinal cord and dorsal root ganglia. (Silverman, et al, 2020)
TRPV1 regulates the gut-brain axis, weight, food absorption, emesis, and colitis primarily in response to endovanilloids and endocannabinoids. Activation of TRPV1 channels can decrease obesity by increasing oxidation of fat molecules or increase risks of obesity-induced chronic inflammation by effects in pancreatic cells, depending on dose of the triggering substance. (Kumar, et al, 2013)
Sodium channels are also frequently seen in nociceptive pain sensors. Inhibitors of them or TRPV1 channels have been tested and negative side effects were a problem for both types due to the widespread distribution and functions of the ion channels throughout the body. (Neurobiology of Disease. pp 855-857) TRPV1 channels are associated with pain and inflammation but also have anti-inflammatory roles suggesting caution is needed with antagonist medications or treatments. TRPV1 null mice had worse inflammation in experimentally induced sepsis, than the wildtype. (Alawi and Keeble, 2009) TRPV1 activation was found protective against oxidative stress for hippocampal cells. (Kumar, et al, 2013)
Modulating herbs have value in restoring balance, promoting the desirable homeostasis, whether an increase or decrease in activity is needed. TRPV1 channels may help protect the brain by regulation of the glutamate receptor and dopaminergic neurons (animal study) or harm it with increased release of substance-P and glutamate at synapses. (Kumar, et al, 2013)
TRPV4 – osmoregulation and metabolism of epoxyeicosatrienoic acid (Arachidonic acid metabolite)
TRP channels can be very specific in their sensing ranges as seen in osmoregulation by TRPV4 channels which react to changes “of even a few mOsmol/kg H2O.” (Tian W, et al, 2009)
TRPV1 and TRPV4 channels, activated by histamine.
Histamine activates TRPV1 and TRPV4 ion channels which activate sensory neurons by producing 12-HPETE, a downstream metabolite of phospholipases A2 (PLA2) and Lipoxygenase (LO), and 12 (s)-HPETE activates TRPV1 channels which cause nociceptive pain. (Table 1, Kumar, et al, 2013) Histamine is activating a chain of events that leads to increased pain and increased release of endocannabinoids from the membranes for the production of prostaglandins in response to the PLA2. This also leads to an increase in free arachidonic acid. (Juan and Sametz, 1980)
TRPV4, TRPC5 and TRPC6 channels, activated by Arachidonic acid.
Arachidonic acid (AA) is a metabolite formed from endocannabinoids released from cell membranes in response to intracellular calcium levels. It is the lipid portion of the phospholipid. Excess arachidonic acid is seen in many inflammatory conditions as PLA2 causes breakdown of phospholipids and release of the arachidonic acid portion or lysophosphatidic acid during the production of eicosanoids.
Endocannabinoids and eicosanoids have a protective role for the brain during acute inflammation. Signaling functions include reducing pain, promoting Nitric oxide or inhibiting increases in Nitric oxide in response to lipopolysaccharides, and modulating calcium entry to NMDA receptors, (McAllister and Abood, 2006), which would be protective of the hippocampus during histamine excess.
Arachidonic acid can accumulate from the release of endocannabinoids from the membrane and resulting breakdown by PLA2, FAAH, and others. It can also accumulate from dietary sources. Chicken fat and broth are a rich source of arachidonic acid.
Arachidonic acid can add to inflammation by activating TRPV4 channels which regulate cell swelling and metabolism of epoxyeicosatrienoic acid (an Arachidonic Acid metabolite). Epoxyeicosatrienoic acid can activate TRPC5 and TRPC6 channels, causing an increase in intracellular calcium and helps with translocation of channels to the membrane in epithelial cells. 20-HETE, another Arachidonic Acid metabolite, can also activate TRPC6 channels. Arachidonic acid also activates TRPV3 channels increasing the activity of cells expressing that type of channel. (Table 1, Kumar, et al, 2013)
Endocannabinoids are released from the membrane in response to intracellular calcium levels which could make inflammatory signals self-perpetuating. Inflammation causes mast cells to degranulate, leading to histamine activating TRP channels to allow calcium into cells, which causes cannabinoid release from the cell membrane, which may lead to more TRP channels on the skin surface, which would lead to more inflammatory reactions from the more sensitive skin.
In a study on hyper-excitable neuromas, annexins A1 and A4 were up regulated compared to the normal cells. Functions of Annexin A1 includes membrane aggregation and inhibiting the mobilization of arachidonic acid and phagocytosis. (Huang, et al, 2008)
TRPC4 and TRPC5 in the kidney, with bitter taste receptors, and bitter tasting polyphenols (- from the game Clue, paraphrased).
Why do we have bitter taste receptors in the kidneys? because when activated they increase the removal of calcium. Alkaloid plant phytonutrients, phellodendrine and coptisine, have been found to activate the renal taste receptors and increase uptake of calcium as a result. The uptake was inhibited by phospholipase C (PLC) inhibitor U-73122. (Liang, et al, 2017) Caffeine is also an alkaloid phytonutrient known to increase calcium excretion. (Chen and Lin, 2020) Bitter taste receptors are team players with TRP ion channels and voltage gated calcium channels within the kidney. (Zhou and Greka, 2016)
TRPC4 and TRPC5 channels also require PLC for activation. TRPC4 required coincident activation by a G coupled receptor and PLC. (Thakur, et al, 2016) Taste receptors are G-coupled protein receptors. (Sanematsu, et al, 2014)
TRPC5 is highly expressed in the kidney on podocytes and is involved in calcium ion influx. Inhibition or genetic deletion of TRPC5 channels reduced filtration barrier injury when lipopolysaccharide (LPS)- or protamine sulfate (PS) was given to induce kidney injury in mouse models. The mice were protected from albuminuria when TRPC5 channels were inhibited or knocked out. (Schaldecker, et al, 2013), (Zhou and Greka, 2016) Providing butyrate protected wildtype mice from kidney injury induced by a single injection of Adriamycin, while those who had been treated with auto-antibodies against the niacin and butyrate receptor GP109 were not protected by the butyrate treatment. GP109 was heavily expressed on kidney podocytes. Providing a prebiotic diet that promoted butyrate production by the gut microbiome was also protective. (Felizardo, et al, 2019)
The functional roles of bitter taste receptors and other sensory receptors located in areas of the body other than the sensory organs is a fairly new area of study. Some medications such as hydroxychloroquine may be acting on bitter taste receptors making it an area of study of interest to pharmacology and nephrologists.
TRPC1, TRPC4 and TRPC5 inhibition by NCAM with glycan polysialic acid attached.
Glycan polysialic acid (PSA) a homopolymer of sialic acid, may also be regulatory of transient receptor potential canonical (TRPC) ion channels TRPC1, -4 and -5. Inhibition of the neural cell adhesion molecule (NCAM) which has glycan polysialic acid (PSA) covalently attached, led to opening of the channels allowing calcium to enter the cortical neurons and CHO cells. (Amores-Bonet, et al, 2022) Polysialic glycan is made up of multiple sialic acids connected together and two polysialyltransferases, polysialyltransferase (PST) and sialyltransferase X (STX), work in coordination to build the homopolymer of sialic acid on NCAM. (Nakayama, et al, 1998) STX and PST are expressed differentially in embryonic tissues versus adult, and within different areas of the adult brain and body. Both STX and PST are involved in polysialic formation within the hippocampus. (Angata, et al, 1997)
It requires the nucleotide UDP and N-acetyl-glucosamine to make sialic acid, and that might be limited functionally during ill health or aging. (Rawal and Zhao, 2021) Suggesting that adequate poly-sialated NCAM helps keep the TRPC channels closed – reducing risk of excess activation by calcium which would lead to release of endocannabinoids from the cell membrane possibly.
- Dietary sources of nucleotides include meats, fish, mushrooms, Nutritional Yeast Flakes, and breast milk – always suggestive that something is essential or semi-essential to have in our diet. (Dancey, Attree and Brown, 2006)
- Dietary sources of N-acetyl-glucosamine (NAG) include the shell of shellfish and insects and is in fungi. (Gaderer, et al, 2017) NAG is available as a supplement and may protective against edematous malnutrition, and inflammatory bowel disease. (Salvatore, et al, 2000, Amadi, et al, 2009) Glucosamine/chondroitin for arthritis is a different form and would not be equivalent chemically for sialic acid production. (Glucosamine, N-Acetyl-D-Glucosamine)
It is not known why stress can lead to over-expression of TRP channels.
In a study comparing normal cells with hypersensitive neuromas of the rat saphenous nerve, while around 200 proteins were upregulated in the neuroma, ion channel mRNA was not increased. This suggests the reason for more TRP channel activity may be due to altered protein expression, local protein synthesis, or topological rearrangement of channels. (Huang, et al, 2008)
Knowing what is causing the pain and knowing how to stop it has more value to patients than simply treating pain. We know over-activation of TRP channels can cause pain signals. We know less about why some people seem to have more activation, or more expression of TRP channels.
Arachidonic acid was discussed earlier as a possible causal factor by increasing translocation of channels to epithelial cell surfaces. The excess breakdown of endocannabinoids in response to histamine and inflammation may be a factor in over-expression of TRP channels. An arachidonic acid metabolite activates TRPC5 and TRPC6 channels that lead to increased translocation of channels to the membrane surface of epithelial cells (discussed earlier). (Table 1, Kumar, et al, 2013) That might result in more channel activity and a hypersensitive skin reaction.
Too much expression of TRP channels may be a factor in pain conditions and is seen in Irritable Bowel Syndrome (IBS) and in rectal hypersensitivity. (Hicks, 2006) (González-Ramírez , et al, 2017 Childhood or chronic trauma can be causal of IBS, a milder form of colitis or Inflammatory bowel disease (IBD). (Sansone and Sansone, 2015) Whether a TRP activator leads to migraines or colitis flare-ups for hypersensitive patients may vary for them based on their current level of overall inflammation and daily stressors. The hypersensitivity may decrease with time once health has been restored for a few years but may remain an intermittent problem for life as health or stress levels worsen again, for child trauma survivors who developed IBS.
Gene alleles affecting nociception may be an individual factor. Retinoid toxicity can be a cause of bowel symptoms. Ulcerative colitis, but not Crohn’s disease, was found to be significantly associated with previous use of the retinoid medication isotretinoin. The association was dose related and more likely for higher doses or for patients taking the medication for longer than two months in a large survey-based study of patients with Inflammatory Bowel Disease. (Crockett, et al, 2010)
Corilagin, a hydrolysable tannin found in other plants than pomegranate, acts as an antagonist of the transient receptor potential vanilloid 1 (TRPV1) channel [54].” (Guerrero-Solano, et al, 2021) Histamine is an activator of TRPV1 channels and can cause pain. TRPV1 channels are also involved in colitis. (Kumar, et al, 2013)
Other possible reasons for over-activity or over-expression of TRP channels.
Gene alleles that may be factors in histamine excess or Retinoid toxicity are in Table 6. Genes that may be involved with histamine excess or Retinoid Toxicity, (incomplete, there are others to add). The Table also has some of my known alleles that impact metabolic pathways, as (n=1) an example person who has had symptoms of histamine hyperexcitability and Retinoid Toxicity and improved with diet changes.
Serotonin and bradykinin:
Chronic itch is a chronic pain condition associated with histamine excess and serotonin excess has been found to be a factor. The serotonin receptor HTR7 gene was found most closely associated with chronic itch in an animal-based study, however over 70 genes were found to be more expressed or more active in lab animals with chronic itch. The gene expression of the HTR7 gene was most active in the mice with the worst symptoms of scratching compared to the mice with the least over-sensitivity. The activity of the TRPA1 receptor was also increased in animals with more symptoms. Increased serotonin levels and serotonin reuptake inhibitors would worsen chronic itch for people with more expression of HTR7. (Morita, et al, 2015)
Serotonin and other “Inflammatory mediators, such as bradykinin…[19, 35]” (Horvath, et al, 2016)can make the TRP channels more sensitive which can lead to increased responsiveness of nerve endings to a smaller amount of activating substance or condition – more Rheumatoid arthritis pain (Horvath, et al, 2016) or itch. (Morita, et al, 2015)
Retinoid Toxicity:
Retinoids cause mast cell degranulation and histamine increase. Retinoid excess could affect gene transcription of proteins transcribed by several groups of receptors and proteins transcribed by the Vitamin D and Thyroid receptors.
“As noted in our review on GWI [41], mast cells are increased in patients with atopic dermatitis and express high levels of retinoic acid receptor-alpha. Retinoic acid (RA) also interferes with the proliferation of skin mast cells and promotes their degranulation, supporting the concept that RA has a pro-allergic and pro-inflammatory-maintaining function in skin mast cells” (Mawson, Croft, 2020)
If Retinoid Toxicity is an underlying problem, then the excess active Retinoic Acid could be causing over-expression of many genes clustered around immune or inflammatory response functions as that is a primary role of retinoid metabolism in addition to eyesight. Variability among patients might be expected as which genes are over-expressed might vary over a broad range. The Retinoic Acid Receptor alone is estimated to be able to transcribe 10-15,000 different genes and their proteins. (Reay and Cairns, 2020) Retinoic acid also activates retinoic acid receptors (RAR), orphan retinoid X receptors (RXR), and peroxisome proliferator-activated receptor beta/delta (PPARβ/δ). Retinoic acid also interacts with the Vitamin D and Thyroid receptors via Retinoid X Receptor (RXR) activation. Excess activated Retinoic Acid (various forms, collectively called retinoids) might lead to increased gene transcription of products affected by any of those four types of receptors in addition to an increase in proteins transcribed directly by activation of Retinoic Acid Receptors (RAR). (Reay and Cairns, 2020)
In a study comparing normal cells with hypersensitive neuromas of the rat saphenous nerve, around 200 proteins were upregulated in the neuroma. Fifty-five were identified which included cytoskeletal proteins, enzymes and proteins associated with oxidative stress. (Huang, et al, 2008)
Methylation dysfunction: Epigenetic changes may be a factor too. Lack of methyl folate can lead to histamine accumulation due to lack of breakdown and may increase risk of epigenetic changes in genes. POTS can be due to epigenetic changes, which means it is reversible, with provision of methyl folate, methyl-cobalamin and choline, and removal of formaldehyde or other volatile chemicals from the living environment. Folate is also needed to break down formaldehyde. Formaldehyde is also a TRP channel activator. (“formalin” (McNamara, et al, 2007) We make our own formaldehyde endogenously when stressed and it is a metabolite of methanol which is a dietary metabolite of the sweetener aspartame. (Hovda et al, 2017) (Walton and Monte, 2015)
For treatment of methanol or formaldehyde poisoning, “folate […] a dose of 50 mg four times a day (every 6 hours) is recommended (Grade III recommendation).” (Hovda et al, 2017) Discussion: Folic acid and folate are mentioned in the article interchangeably, but folic acid may not be consistently helpful in research results because the methyl folate form is needed to help breakdown formaldehyde and not all people methylate well. Whether genetically, or age or dysfunction related, metabolic pathways may not be efficient. Folic acid is an unmethylated synthetic form of methyl folate. The typical supplements of folate available are 400-1000 mcg (0.4-1 milligram) as the nutrient guideline is 400 mcg. Fifty milligrams of folic acid may not be helpful even for someone who can methylate normal amounts of the B vitamin.
Capsaicin topical treatments:
Treatments using capsaicin to over-activate TRP channels to a point of numbing them, may be a flawed approach if the increased activation to the point of numbing leads to more expression of TRP channels in some people (Mayoclinic) which would add to pain in the future. If the size of your tummy is an emotionally painful subject, visceral adipose tissue was reduced with topical capsaicin treatment in an animal-based study. (Lee, et al, 2013) Capsaicin activates TRPV1 channels which increase fat oxidation, (Kumar, et al, 2013), discussed more in a later section.
Stress and overactivation or overexpression of TRP channels:
Oxidative stress chemicals also activate TRP channels that send pain signals. Many common seasonings seem “spicy” because they stimulate, while too much would overstimulate and cause a burning or caustic sensation. Oral therapeutic treatments have value in allowing the bitter taste receptors to help guide individual dosing needs. Bitter taste receptors and odor receptors are found in functional roles in various tissue types throughout the body in roles other than sending taste or odor signals to the brain. Taste receptors for bitter tastes are 10,000 times more sensitive than for sweet tastes which helps guide us to a therapeutic amount of the bitter tasting and medicinally valuable and/or potentially toxic phytonutrients. Dose makes the difference between benefit and harm. Bitter taste receptors are discussed more in a later section.
Chronic stress seems to lead to an over-expression of TRPA-1 channels in some conditions, which may remain for life (IBS/colitis) or may occur due to a variety of gene differences in the case of chronic itch – discussed earlier. We all tear up with the fumes of raw onion (allicin), (Bautista, et al, 2005) (Macpherson, et al, 2005) or mustard gas, or grating raw wasabi or horseradish, (allyl isothiocyanate). (Jordt, et al, 2004) People with Irritable Bowel Syndrome might feel pain and a sudden need for the bathroom after eating mustard or other TRPA-1 activating spices like black pepper, horseradish, ginger, or turmeric. Cinnamon (cinnamaldehyde) or mint (menthol), (Namer, et al, 2005), may cause migraines in people with overactive or too much expression of TRPA-1 channels. Formaldehyde, chemical name of formalin, may be from smoke, smog, vinyl furnishings, or can be endogenously made in response to stress, and it can add to pain by activating TRPA-1 channels. (McNamara, et al, 2007)
Emotional dysregulation, worsened by histamine excess, further increasing stress levels:
Histamine hyperexcitability, and self-harm urges, may occur daily when standard foods are being eaten. Itchy skin, may be similar to an over-agitated mind – how can you scratch that itch? The emotional over-activity can lead to worse inflammation symptoms the next day. Eating histamine foods, or having significant stress, or exposure to strong EMF, and other triggers like an amusement park ride or strobe-light action movie, can degranulate mast cells and cause histamine excess and then histamine excess symptoms return. Symptoms therefore may fluctuate and seem random rather than diet and lifestyle based. The day after an episode of more severe emotional dysregulation may leave a person with flu-like symptoms of inflammation. Hippocampal damage would likely be accruing over time and worsened with more extreme episodes.
Avoiding the cause of mast cell degranulation can help prevent the histamine excess. Avoiding dietary food sources and environmental irritants is needed though. The list of things of inflammatory things to avoid is extensive but consistently avoiding them can restore the person to their rational self. It is not a ‘cure’ though. Return of symptoms occurs shortly after or the next day after a triggering event or meal.
If Retinoid Toxicity is also a problem, then the list of foods to avoid is even longer and again, symptoms might fluctuate based on the vitamin A and carotenoid content of what the patient had for dinner last night (discussed in the section about Table 2. Potentially Inflammatory Foods).
Post-Translational modification (PTM) of proteins.
A study on CNS hyperalgesia found “post-translational modification (PTM) of proteolysis or phosphorylation” to be involved in the pain condition rather than increased mRNA expression of the three proteins that were identified. (Fujisawa, et al, 2008) Post-translational modification of proteins is also seen in autoimmune Rheumatoid arthritis. Auto-antibodies form against the modified proteins which leads to autoimmune damage to healthy proteins. (Vasudevan, et al, 2021)
“Early diagnosis of RA is necessary to manage the aggressive symptoms. Currently, Rheumatoid factor (RF) and anti-citrullinated cyclic peptide (Anti-CCP) are considered as biomarkers to diagnose RA. Besides citrullination, several other PTMs are also involved in the generation of autoantibodies, such as carbamylation, glycosylation, glycation, acetylation, ubiquitination, proteolysis, phosphorylation, and lipidation.” (Vasudevan, et al, 2021)
Nociceptive pain is considered acute, traumatic injury related, typically, while neuropathic pain may be chronic over-activity of pain signaling nerves. Post-translational modification of sodium voltage gated channels modifies their activity in neuropathic chronic pain syndrome. (Laedermann, et al, 2015)
“Inflammatory pain is due to the modification of the chemical environment surrounding nociceptive neurons and the accumulation of several factors secreted by recruited non-neural cells, such as mast cells, macrophages, neutrophils, inflammatory cells, fibroblasts and keratinocytes, as well as by the nociceptive neurons themselves. These factors are of diverse origins but include protons (H+), nerve growth factors (NGFs), cytokines (such as IL-1β, IL-6), tumor necrosis factor alpha (TNF-α), prostaglandins (PGE2), several neurotransmitters (serotonin, ATP) and peptides (bradykinin, substance P, CGRP). This mixture is commonly referred to as “the inflammatory soup” (Basbaum et al., 2009), and will increase spontaneous neuronal firing, usually decrease the threshold of nociceptive neurons and increase firing in response to suprathreshold stimuli. The mechanisms by which inflammatory pain increases pain transmission include the activation of kinases that phosphorylate membrane channels and receptors, which subsequently alter their function, and the genetic regulation of primary sensory neurons (Woolf and Costigan, 1999). Inflammatory pain, by the virtue of central sensitization, is also accompanied by the local loss of inhibition (Julius and Basbaum, 2001) and enhanced postsynaptic transmission (Galan et al., 2004).” (Laedermann, et al, 2015, CC By the authors)
What makes PTM more likely? Oxidative stress levels, mitochondrial dysfunction, high fructose diet, general malnutrition, lack of endocannabinoids, lack of CoQ10. That would be a different paper – or would it? (Related webpage, PTM also is a causal issue in demyelination conditions: effectivecare.info/Demyelination, or more extensive document.)
Endocannabinoids and the neuropathic pain of noise hyper-sensitivity.
An influx of sodium might depolarize a nerve cell and send a nerve signal which might be perceived as pain or something else depending on the function of the cell or channel. Too much activity of a sensory signal might be perceived as sensitivity to noise or a constant ringing tinnitus that is CNS derived rather than being due to damaged Hair Cells within the inner ear. Reducing neuroinflammation may help reduce the pain of sound signals that continue too long, a problem seen in patients with autism and Alzheimer’s dementia. Hawthorn extract was found helpful for neuroinflammation in an animal-based stroke model, reducing cytotoxic T-cells and inflammatory cytokines. Beneficial Tregs and IL-10 levels were increased. (Elango and Devaraj, 2010) Phytonutrient preparations frequently are made with proprietary blends that may have synergistic benefits. Blends of herbs that balance any negatives within the mix is a goal for Traditional Chinese Medicinal remedies.
Lack of endocannabinoids may also be a cause of noise hypersensitivity. An overactive startle reflex may also indicate a deficiency of cannabinoids as they are needed for synaptic regulation, to inhibit nerve signals after a time lapse. Imagine a doorbell buzzing . . . what if it never stopped? or only stopped after two minutes of continual buzzing? That would likely seem painful. Prepulse inhibition (PPI) is a phrase used to describe our normal ability to dampen down a startle response if prewarned that a loud noise is about to happen. It is common in both autism (Erturk, et al, 2016) and schizophrenia to have a delayed PPI, and be over-startled, but the mechanism of action seems to be slightly different. (Madsen, et al, 2014)
Olanzapine helped improve the PPI response in schizophrenic patients. ((Declan, et al, 2008, viewable at ScD) The medication reduces breakdown of cannabinoids and may cause overeating and weight gain as a side effect. Using CBD drops has been helpful for restoring a more normal startle reflex if lack of cannabinoids is involved. (Pedrazzi, et al, 2015)
Other drugs that make the PPI worse (in animal-based research), increasing a startle reaction even when a noise is expected, include: NMDA antagonists, dopamine agonists, serotonin receptor agonists. It is also seen with varied neurodevelopmental conditions and in transgenic mouse models of schizophrenia. (Pedrazzi, et al, 2015)
What might help prevent pain from mast cell degranulation and histamine?
Overview:
Self-calming techniques:
Disrupting the pain and inflammatory signals can be possible with self-calming techniques. See Table 4: Counseling Strategies for Coping with Urges to Self-Harm, for an example of patient guidance for distracting from self-harm urges. (Walsh, 2006)
Dietary changes:
Avoiding TRP activators, histamine food triggers and vitamin A/carotenoids if Retinoid Toxicity is also a problem, are all necessary to stop the chronic inflammation and calm over-sensitive TRP channels. Table 2. Foods Ranked by Potentially Inflammatory Categories, also has other food categories that may be inflammatory for some people, or are inflammatory in general. It also has a column to show whether a food is otherwise Nrf2 promoting. This Table is discussed in a later section.
Lifestyle changes:
Moderate pace for physical and emotional stress: and pacing activity, avoiding the physical stress of over-exertion, and saying no thanks to the extreme sport or amusement park ride may be needed.
- Avoid temperature extremes: wearing layered clothing to easily adjust to temperature changes,
- Avoid pressure changes: position and pressure internally or externally can affect IBS/colitis – for example, amusement park rides, yoga poses, or laying on your side. Raw vegetables or large servings of raw fruit might lead to internal gas, and pain in the hypersensitized gut. TRP channels are activated by the pressure change and it leads to an influx of fluid into the intestines and a sudden watery bowel movement. Dehydration may become a risk as electrolytes and fluid are lost. Similar symptoms can occur with the dietary or temperature extremes.
- Avoid strong EMF fields or in sleep areas.
Those are a few ways to reduce activating TRP channels. Table 3. Self-Care Patient Guidance for ME/CFS, hyperinflammation, Retinoid toxicity and/or histamine excess, is written as an example of patient guidance or talking points for helping reduce inflammatory causes of TRP channel activation or mast cell degranulation.
Maintaining a healthy weight – pomegranate and zinc can help.
Bitter tasting phenols in fruit may promote weight loss, varying with the type of fruit. Pomegranate is particularly helpful and bitter taste receptors (Tas2rs) may be involved.
Bitter tasting phenolic compounds have been found to have weight loss/anti-obesity benefits including: resveratrol, caffeic acid, naringenin, proanthocyanidins, catechins, and cyanidin. (Sharma, et al., 2016) Proanthocyanidins, and catechins are present in pomegranate and chlorogenic and caffeic acid, both gallic acids.(Mahmoud and Ibrahim, 2013) Caffeic acid (Frank, et al, 2007) and many other pomegranate phytonutrients are bitter tasting.
Pomegranate juice was more effective compared to an extract for improving glycemic response with a high-glycemic index food. (Kerimi, et al, 2017)
Bitter taste receptors (Tas2rs) increase glucose tolerance, improve weight and dyslipidemia, and decrease insulin resistance, in part by stimulating production of the hormone glucagon-like peptide 1 (GLP-1); animal-based study on hops isohumulones. (Kok, et al, date) GLP-1 promotes satiety through interaction with ghrelin and leptin, resulting in inhibition of glucagon and increased insulin secretion. (Ronveaux, et al, 2015) Leptin also stimulates GLP-1 and GLP-1 is low in obesity, leptin resistance is suggested to be a factor. (Anini, et al, 2003) Lack of bitter taste receptors due to zinc deficiency might be a factor, and/or the lack of bitter tasting phytonutrients in processed foods. Processed foods tend to have had the bitter tasting phytonutrients removed to increase consumer acceptance.
Leptin levels fall during fasting or weight loss, and the decrease signals to eat, and then regain may occur. Maintaining leptin levels helped weight (animal study). (Ahima, 2008) Elevated leptin levels and leptin resistance are associated with obesity.
Zinc deficiency effect gene transcription of taste receptors and other genes.
Zinc deficiency would cause a lack of bitter taste receptors as Zinc finger proteins are needed for gene transcription of odor and taste receptors, (Sekine, et al, 2012), and many other proteins including genes transcribed by other nuclear transcription factors. (Mackeh, et al, 2018) Zinc deficiency can impact gene transcription by retinoid X receptors (RXR) and 27 other types of gene transcription factors, so deficiency of zinc can negatively impact stem cell differentiation in neonatal or adult neurogenesis. (Morris and Levenson, 2013)
The elderly and chronically ill may have zinc deficiency as an underlying causal factor, as bitter taste receptors on immune cells and within the kidney and elsewhere in the body affect health. Supplementation at higher than standard recommendation may be needed for at least three months to see improvement in taste and odor sensation, (Kodama, et al, 2020), and other chronic symptoms may improve also.
Pomegranate fruit or peel products, other Nrf2 promoting phytonutrients and foods:
Adding Nrf2 promoting foods like pomegranate can help prevent degranulation of mast cells. Taking pomegranate products could also help inhibit mast cells and prevent more histamine from activating more TRP pain channels. Phytonutrients in pomegranate also can reduce long-term risks of damage to the liver, kidney and brain, (See: Table 7. Health benefits observed with pomegranate, and Table 8. Phytonutrients in pomegranate), which are risks from histamine excess and/or Retinoid Toxicity, (See: Table 1. Symptoms) Preventing the pain in the first place would be more efficient than taking pain medications on a chronic basis which can lead to rebound headaches, digestive discomfort, and liver damage.
Field tests suggest 3-4 ounces of juice or seeds can be calming within 20 minutes, and foods containing pomegranate peel also help but digestion may slow down the calming response (Personal experience, n=2). Nrf2 promoting herbs and mitochondrial support nutrients can help reduce inflammation which otherwise adds to mast cell degranulation. Methyl folate may be needed to help metabolize histamine. Avoiding histamine foods or allergy trigger foods can help prevent excess accumulation of histamine from the gut where many mast cells are located.
Pomegranate whole fruit extract may help more than single phytonutrient isolates.
Whole fruit products may have more health benefits than single isolates of pomegranate. Modulation of the microbiome may be involved and synergistic effects of pomegranate peel extract phytonutrients. (Viladomiu, et al, 2013), (Zarfeshany, et al, 2014) Much of the research regarding health benefits of pomegranate has focused on the ellagic acid component, however benefits are seen with juice and juice made with the whole fruit, or peel extracts rather than isolates. A study comparing a supplement of ellagic acid to an equivalent portion of pomegranate juice found similar absorption but more health benefits from the juice, suggesting other bioactive phytonutrients provide some of the health benefits. Bioavailability and bioactivity of free ellagic acid compared to pomegranate juice, (Long, et al, 2019)
Healthy Circadian Cycle:
NF-kB inhibiting phytonutrients are also Nrf2 promoting phytonutrients as the two pathways share a circadian cycle Clock protein. Restoring a healthy circadian cycle with sleep/wake, dark/full spectrum light strategies is also a need as Nrf2 activity reduces inflammation and pain and is involved in DNA damage repair. Reducing inflammation is needed to reduce breakdown of endocannabinoids as that leads to activation of TRP channels, increased calcium entry into cells, edematous changes, and increased expression of TRP channels on cell surfaces may result – leading to increased sensitivity to TRP activators into the future.
Magnesium (topical or chelated sources may be needed with GI symptoms or in chronic illness):
Magnesium helps prevent opening of some TRP channel types and is needed for apoptosis. Plant polyphenols from pomegranate and other plants help reduce the inflammatory signaling by inhibiting the NF-kB pathways and promoting the Nrf2 pathways which help with DNA damage repair, detoxification and growth of cells; acting as antioxidants and iron chelators and reducing oxidative stress damage from free radicals or excess free iron; modulating Nitric oxide levels and immune function by affecting cytokine balance; providing mitochondrial and microbiome support; and stabilizing proteins or supporting endoplasmic reticulum function for removing misfolded proteins. Plant polyphenols and magnesium help prevent cell senescence and support apoptosis.
Magnesium is likely needed to help block calcium entry for some types of TRP channels, (Srebro, et al, 2016), – or TRP channel activation may occur due to food agonists, osmomechanical pressure changes, excess acidity, sunlight, EMF, or spending time in temperatures below 40’F or above ~80’F temperature or having a sudden change in temperature – hot summer to over-air-conditioned chill.
Too much pressure and the TRP channels act as valves and leak fluid rather than letting the cell or marine species burst. Pain and puffiness are companions that may both be reduced by adequate magnesium. Excess magnesium sulfate injected peripherally can cause pain via TRPV1, TRPV4 and TRPA1 channels, while it has an anti-nociceptive effect at a systemic level. (Srebro, et al, 2016) Delphinidin is a phytonutrient in pomegranate peel that includes four atoms of magnesium within its molecular structure. Delphinidin has been found beneficial for chronic dry eye conditions in a trial with a product using the Maqui berry (Aristotelia chilensis) as the phytonutrient source. (Yamashita, et al, 2018) Delphinidin is an anti-inflammatory Nrf2 promoter and NF-kB inhibitor and seems protective against misfolded protein conditions as an allosteric modulator. See Table. Pom phytonutrients. However more magnesium would likely be needed to help inflammatory conditions than from delphinidin in pomegranate peel or Maqui berries.
Glycine and Serine, Inositol, other inhibitory nutrients in addition to magnesium:
The free amino acids glycine and serine have inhibitory roles in some types of channels or receptors. Inositol and other nutrients also may have calming effects for an over-excited brain and body.
Cannabinoids, in combination, inhaled may be important for mast cell inhibition compared to digestive sources:
More controversially, inhaled THC and CBD, in combination, also inhibits mast cells from degranulating. Inhaled sources bypass changes that occur in the digestive process. The mucosal spray Sativex TM or similar products could be tested for efficacy with histamine excess. Gene alleles affecting endocannabinoid metabolism such as BHMT would be a risk factor for histamine excess. See Table. Genes. Antiphospholipid Syndrome may also add to histamine risks, as it causes autoimmune breakdown of endocannabinoids and leads to symptoms of cannabinoid deficiency. Antiphospholipid Syndrome has been seen in LongCovid patients and can be a causal factor for the dysautonomia condition Postural Orthostatic Tachycardia Syndrome (POTS) which is also seen in LongCovid and comorbidly with ME/CFS. Ehlers-Danlos Syndrome (EDS) also is a condition that may affect endogenous cannabinoid production and an external source may be needed.
Mitochondrial support nutrients and high dose niacin (flush type), resistant starch/butyrate:
With additional mitochondrial support nutrients, methyl B complex and a good trace mineral mix, CoQ10, alpha lipoic acid, cysteine, and others help the mitochondria provide us energy and reduce oxidative stress. Nrf2 promoting foods help by promoting glutathione production. Other nutrients needed for the Citric Acid Cycle, or which play other roles for mitochondria, are listed after Table 5. Nutrients depleted by psychiatric medications; risk factors for schizoaffective disorder; and mitochondrial support nutrients – all three overlap.
~~ And included here:
Vitamin A is needed by mitochondria, (Chiu, et al, 2008), while excess activated retinoids are harmful to mitochondria. (de Oliveira, 2015) Hyponatremia or low calcium (Killilea and Killilea, 2022) or excess sodium (Mehrer, et al, 2022) or excess calcium (Pivovarova and Andrews, 2010) would cause mitochondrial dysfunction.
The Citric Acid Cycle requires these nutrients, free amino acids and cofactors:
- B vitamins: B1 (Thiamin), B2 (Riboflavin), B3 (Niacin), B5 (Pantothenic acid), B6 (Pyridoxine), B7 (Biotin), B9 (Folate).
- Minerals: Mg++ (Magnesium), Mn++ (Manganese), K+ (Potassium), Zinc, Iron, Copper, Sulfate.
- Amino acids: Carnitine (derived from lysine), Cysteine.
- Antioxidants: CoQ10, Glutathione, Alpha-Lipoic Acid (ALA).
- From a graphic labeled by Dmitry Kats, PhD. Additional links at: https://transcendingsquare.com/2021/04/30/niacin-may-help-reduce-chronic-migraines/
B12 has a coenzyme role in mitochondria. (Janssen, et al, 2019) Inositol is an inhibitor of AMPK and therefore is protective against mitochondrial fission. (Hsu, et al, 2021) The Vitamin D Receptor has a regulatory role over mitochondrial function. (Ricca, et al, 2018) Vitamin C is protective of mitochondria as an additional antioxidant, excess could be a pro-oxidant against cancer cells. (Singh and Vir, 2010) Vitamin K2 has a protective and regulatory role over mitochondria apoptosis and biogenesis. (Tang, et al, 2022) Essential fatty acids are essential for mitochondrial membranes. (Sullivan, et al, 2018) Selenium is protective of mitochondria and promotes biogenesis of mitochondria. (Mehta, et al, 2012)
~~
Similar to capsaicin increasing fat oxidation by TRPV1 activation, (Kumar, et al, 2013), niacin and butyrate also can increase removal of inflammation by affecting mitochondrial energy production. The mechanism of action is different – activation of GP109 receptors leads to mitochondrial oxidation being decoupled from ATP production and the energy is released as warmth instead, similarly to brown adipose tissue. High dose niacin, 1000 mg three times a day, has been found helpful and safe for patients with schizophrenia in a clinical trial. Gout was not a complication and pre-existing cases could use a lower dose of nicotinic acid/niacin. Nicotinamide did not help the patients equivalently to the niacin flush form. (Hoffer, 1971)
Butyrate’s protective role in kidney health was discussed earlier in the section on TRPC4 and TRPC5 and bitter taste receptors. The niacin/butyrate GP109 receptor and taste receptors are G-couple protein receptors, crossing the membrane and performing actions on the cell’s interior.
- PPAR beta/delta receptors can activate fat burning in mitochondria by fermentation instead of Citric Acid Cycle oxidation and can be activated by 9-cis-Retinoic Acid. High saturated fat diets also cause the switch to fermentation of fat. This is meant to be temporary as the diet balance fluctuates, not a long-term change as seen in chronic conditions of modern life.
Mitochondrial dysfunction and failure to produce acetyl CoA is seen in ME/CFS. The reason why is not known but could be due to Retinoid Toxicity. Lack of nutrients and cofactors needed in the Citric Acid Cycle can be a factor and a high saturated fat diet can also cause a shift in mitochondrial energy production to fermentation instead of use of the more productive and less waste producing Citric Acid Cycle.
Retinol promotes the Citric Acid Cycle (Acin-Perez, et al, 2010) but Retinoic Acid could be blocking it. Retinoic acid excess could be a reason that CoA production is blocked. (Tyagi, et al, 2011) (Zhang S, et al, 2014, Fig. 2) Over-conversion of active Retinoic Acid in the liver leads to a deficiency of the inactive retinol form of vitamin A. (Mawson, Croft, 2020)
The ability to use the Citric Acid Cycle can be turned off by Retinoic acid activated PPAR beta/delta receptors, (Reay and Cairns, 2020), inhibiting PDK which then prevents production of Acetyl CoA, which is needed for the cycle to occur within mitochondria. (Tyagi, et al, 2011)
Diet with moderate to low saturated fats:
Added complexity, a high saturated fat diet is the normal cause for the PPAR beta/delta inhibition of PDK and the Citric Acid Cycle by limiting CoA production . . . which blocks the Citric Acid Cycle from functioning, and the mitochondria switch to using fat for energy. (Tyagi, et al, 2011) (Zhang S, et al, 2014, Fig. 2)
This PDK switch is a standard part of metabolism and would be lifesaving when food was scarce – a rapid switch to using whatever type of energy was most available at the time. In modern life saturated fats can be a significant part of the diet. Using fermentation for energy production is more inefficient for energy needs though, and produces more waste and lactate build up from the accumulating pyruvate. Elevated pyruvate levels are seen in ME/CFS. (Anderson and Maes, 2020)
Identifying dietary and lifestyle histamine or mast cell triggers.
Dietary triggers for overly sensitive people are numerous and varied individually. Favorite foods may be the problem, because they are favorite, and the gut is exposed daily to the proteins, increasing allergy or autoimmune risks, or another inflammatory sensitization. Table 2 is a snapshot of a much larger database that physicians and patients need to have created, to more easily identify dietary triggers of inflammation. See: Table 2. Foods Ranked by Potentially Inflammatory Categories, NF-kB promoting if sensitive; and Nrf2 promoting status otherwise* – healthy if not individually sensitized and the product was grown organically. Table 2 includes categories of potentially inflammatory foods, which otherwise may be healthy foods for people who are not overly sensitive. The table includes categories for foods which may be harmful individually or in general: Histamine foods, Vitamin A/carotenoids, Oxalates, Lectins, TRP activators, common Food Allergens, common Molecular Mimicry autoimmune proteins, Glyphosate, and Glutamate. An additional column for Nrf2 promoting is to show that if tolerated individually, in moderation, without agricultural contaminants, the food item is healthy.
Lifestyle factors would be an additional group of inflammatory concerns. See Table 3. Self-Care for lifestyle guidance for patients.
The focus of foods listed in Table 2 is on TRP channel activators rather than histamine trigger foods or vitamin A and carotenoids, as this article is about nociceptive pain and TRP channels are so closely involved with pain signaling. A larger database accessible with a phone application that includes most typical foods would be needed.
If a patient is over-converting Vitamin A and carotenoids to Retinoic Acid, then thoroughly restricting all dietary sources of vitamin A and carotenoids and active Retinoic Acid (in foods like liver) is needed. There would always be some intake from dark green veggies, but as long as it isn’t full servings inflammatory symptoms might not occur the next day (personal experience, n =1).
The topic of TRP activators is also new from a therapeutic diet perspective. As patient (n=1), I had to learn what various spices, CBD, osmo-mechanical pressure changes, and getting too cold or too hot, all had in common – TRP channel activation. Hot pepper, black pepper, horseradish, ginger, turmeric, mustard, cinnamon, cloves, nutmeg, mint, and vanilla are TRP activators and may cause migraines or IBS/colitis symptoms depending on dose and the individual sensitivity. Vanilla seems more calming of an TRPV1 agonist than the others. Mint is recommended for headaches but eventually was a trigger for migraines for me (n=1), cinnamon still is, but I can tolerate small amounts of mint now having reduced my level of inflammation for over two years. TRP activating spices are good in moderation and painful in excess.
Many types of TRP channels exist with varying agonists and those details are not included in Table 2 – it is a snapshot to get an idea of the size of the problem of identifying possible food triggers for individual patients or their health care team.
From Table 2, a few non-food items are included, TRP activating chemicals include: Histamine, Dopamine, Leptin, Arachidonic acid, Glutamate, cytokines, Substance P, and many others, (See: Table 1, Kumar, et al, 2013), other hormone agonists include 1, 25, dihydroxy cholecalciferol-vit D and curcumin, a Vitamin D Receptor agonist found in turmeric. Also, “…estrogen, androgen, testosterone, cortisol and many other steroids (Table 1)” (Kumar, et al, 2013) ) are TRP channel activators, which suggests that estrogen mimetic chemicals may also add to chronic inflammation or other metabolic dysfunction.
Pomegranate phytonutrients and pharmaceutical and other applications.
Pomegranate peel phytonutrients can act as a flocculent and adsorb other chemicals including nanoparticles and minerals with a range of valences (delphinidin, EGCG, and other catechins, hydrolysable tannins). They also may act similarly to cofactors and stabilize the reaction of an enzyme or promote or inhibit a ligand from entering a receptor. Pomegranate peel is used in the production of gold and silver nanoparticles for medical (Nasiriboroumand, et al, 2018), (Yang, et al, 2016), (Monira, et al, date), (Nadagouda, et al, 2014), (Rao, et al, 2013) and industrial purposes. See Table 9. Pharma and Topical applications, and Table 11. Industrial applications with pomegranate peel. Lavender has been used in the production of a medically beneficial zinc nanoparticle (Saadatmand, et al, 2021) and pomegranate peel should bond well with a +2 ion. Zinc deficiency is common among the elderly and immune deficient and affects microbiome health. Combined products can aid the body in many ways, delivering needed nutrients or fragile phytonutrients.
Combinations of pomegranate rind extract with copper or zinc enhanced the antimicrobial benefits, from a review article with extensive Tables of microbial species that pomegranate rind extract (PRE) was trialed against, with dosages used and extraction method. (Celiksoy and Heard, 2021)
Hydrolyzable tannins, delphinidin, and other phytonutrients in pomegranate peel bind with minerals and other molecules well. Dissolving kidney stones has been trialed in simulated conditions. (Sree Varicola, et al, 2018)
Pomegranate extract may have value as a carrier for other chemicals. Research with topical applications of pomegranate peel extract or juice have shown benefits for skin health, (Baccarin, et al, 2017), (Fawole, et al, 2012), (Nokinsee et al, 2015), wound healing, (Nirwana, et al, 2017), and anti-microbial action (HIV-1, (Neurath, et al, 2004), and Herpes simplex virus, (Houston, et al, 2017), oral bacterial (Aparecida Procópio Gomes, et al, 2016) and fungal species, (de Oliveira, et al, 2014), (Madugula, et al, 2017)). Production of phospholipid liposomes may also be a use for the phospholipid content of pomegranate seeds left after juice production. Liposomal formulation of the isolate punicalagin has been trialed. (Vora, et al, 2015) See Table 6: Topical and Pharmaceutical trials.
Punicaligin is a hydrolysable tannin and is a large molecule that typically metabolizes during digestion but is beneficial against cancer. Pomegranate products have shown efficacy against colon cancer possibly due to the more direct contact, (Richmond, L.E.2018), making liposomal preparations a promising therapeutic route. Use of punicalagin significantly reduced cell proliferation and increased apoptosis of osteosarcoma cells. The mechanism of action was likely inhibition of NF-kB signaling. (Huang, et al, 2020)
Pomegranate is a sustainable crop and the rind is potent, making it a valuable crop.
Pomegranate is a drought tolerant plant that can tolerate salty soil, but the commercially available cultivar needs a long growing season and not too much rain. If harvesting pomegranate peel is the goal rather than saleable fruit, then a smaller cultivar with a shorter growing season might be an acceptable substitute which could increase the areas where pomegranate could be cultivated for use of the peel. Smaller fruit have a larger ratio of outer peel to inner pith which might affect the crop goals. The outer peel is more potent but has a higher tannin ratio making it inedible except as tea or extract or capsule amounts, while the inner pith is a functional food item with beneficial pectin and other fiber in addition to tannins in a more tolerable amount. Use minced in similar amounts as a couple garlic cloves in a pot of soup. Moderate dosing is needed. Excess would be a diuretic. Functional foods should be tasty but not so tasty that it promotes over-eating – not a candy or cookie or cracker where eating only one or a few may be a challenge.
For recipe creation ideas see what the industry has been experimenting with: Table 10. Research with pomegranate as a food preservative or ingredient.
Preparing whole fruit for peel use would be more labor intensive to separate the fruit, inner pith, and outer rind, however the three parts are usable in different ways. Outer rind could be used for extracts or tannins, the inner pith can be used directly in functional foods, the arils could be used fresh or frozen, or made into juice and the seeds used to make phospholipid liposomal therapeutics or be made into essential oil.
Discussion: Multifactorial problems require multifactorial solutions.
Self-care is not easy in a busy world, and it is more difficult with mental health problems or physical pain and fatigue. Patients suffering from such a varied and complex problem will need a complex solution that would be challenging for a dietitian (*lived experience, n=1) to cope with. Mixed histamine reducing herbal products are available on the market. Adding pomegranate peel extract or urolithin A or B (gut metabolite of pomegranate) to a mixed product with mitochondrial support nutrients, Hawthorne, Nettle, or other herbs, might help provide patients, staff, parents, and individuals with a calming strategy. Reducing the severity of mental symptoms of histamine excess might help restore enough function to be able to work on other lifestyle and dietary factors that might be adding to an individual’s symptoms.
Screening with lab tests might be misleading compared to a Therapeutic Trial – does a serving of pomegranate, quercetin, or luteolin help calm a patient’s symptoms? Elimination diets are also helpful to see if diet is a causal factor and would also be a Therapeutic Trial of the recommended diet. If it works – just continue. Would following a low histamine diet for a month, or a few, lead to a reduction in symptoms? If not, would restricting vitamin A and carotenoid foods help more? Are TRP channel activators, oxalates, lectins, or other food ingredients inflammatory?
Screening questionnaires may be helpful as the list of histamine excess symptoms and Retinoid Toxicity symptoms are not exactly the same, and both include some unusual symptoms other than congestion, fatigue, and edema. Endocannabinoid deficiency generates a third list of potential symptoms or diagnoses frequently associated with lack of cannabinoids or imbalance (schizophrenia).
Resources for cognitive therapy techniques are included in the Tables as the danger to the patient during histamine excess can be severe and immediate coping skills can be lifesaving during impulsive and irrational moments. Practice and having a plan discussed with a trusted authority can be the most necessary tool at a time of need and then the bottle of calming pomegranate may be a second step.
Genetic screening or protein expression testing might be helpful as the impact of excess Retinoic Acid can impact many genes and proteins. It would be a teratogen and could affect the DNA of developing cells such as sperm. If 9-cis Retinoic Acid is preventing production of Acetyl-CoA by activating PPAR leading to inhibition of PDK, then ongoing mitochondrial dysfunction would occur. Stopping the excess retinoids would be needed to restore mitochondrial use of the Citric Acid Cycle – and/or stopping a diet balance high in saturated fats.
Adequate niacin and resistant starch for butyrate production by a healthy microbiome fed with adequate zinc is also an apparent need. More research is needed regarding the TRPC4 and TRPC5 channels in kidney podocytes and the role of butyrate in their regulation. Endocannabinoid breakdown due to inflammatory signaling may be an underlying factor between some of the comorbid conditions.
~
Tables:
- Table 1. Symptoms of histamine excess and of Retinoid Toxicity.
- Table 2. Foods Ranked by Potentially Inflammatory Categories, NF-kB promoting if sensitive; and Nrf2 promoting status otherwise* – healthy if not individually sensitized and the product was grown organically.
- Table 3. Self-Care Patient Guidance for ME/CFS, hyperinflammation, Retinoid toxicity and/or histamine excess.
- Table 4: Counseling Strategies for Coping with Urges to Self-Harm.
- Table 5. Nutrients depleted by common psychiatric medications and nutrients that may be deficient or imbalanced in patients with schizophrenia/schizoaffective disorder.
- Table 6. Genes that may be involved with histamine excess or Retinoid Toxicity.
- Table 7. Health benefits observed with pomegranate.
- Table 8. Phytonutrient content of Pomegranate products and extraction methods.
- Table 9. Topical and Pharmaceutical trials with Pomegranate products.
- Table 10. Research with pomegranate peel as a food preservative or ingredient.
- Table 11. Industrial applications with Pomegranate peel.
- Table 12. Potential Causal factors for histamine excess or Retinoid Toxicity.
Author Notes:
Jennifer R Depew, RD, is unaffiliated with any organization. She has previous career experience in public health as a prenatal and lactation counselor and agency director. Personal health problems led to learning how to solve them. Personal information is shared in this paper as an n=1 case study example of someone who has suffered daily pain and fatigue for decades and who has multiple gene alleles affecting metabolism. Chronic Fatigue and fibromyalgia like symptoms were problems along with severe migraines, prior Epstein-Barr viral infection could have been a causal factor.
Disclaimer: This information is provided for educational purposes within the guidelines of Fair Use. It is not intended to provide individual guidance. Please seek a health care provider for individualized health care guidance.
